doi.org/10.20986/revesppod.2025.1747/2025
REVIEW
Clinical and functional effectiveness of posterior leg muscle lengthening: a systematic review
Efectividad clínica y funcional del alargamiento de la musculatura posterior de la pierna: revisión sistemática
Rafael Rayo Martín1
Marta Andrade Sánchez2
Alberto Rayo Martín3
Ana M.ª Rayo Pérez1
1Universidad de Sevilla. España
2Práctica privada. Sevilla, España
3Clínica Rayo. Arahal, Sevilla, España
Abstract
Introduction: Posterior muscle lengthening is a surgical intervention used to treat equinus and various conditions related to limited ankle function. The objective of this article is to evaluate the effectiveness and safety of different posterior muscle lengthening techniques (including Vulpius, Baumann, Strayer, Hoke, Z-plasty, Baker, Barouk, and Silfverskiöld) through a literature review.
Material and methods: A systematic review of scientific articles published up to 2024 was conducted, selecting those that evaluated the clinical, functional, and surgical outcomes of posterior leg muscle lengthening techniques. Experimental and clinical studies, as well as reviews that provided quantitative data, were included. In all cases, methodological quality and risk of bias were assessed using tools adapted to the design of each study.
Results: Most studies reported significant improvement in ankle dorsiflexion and pain reduction following muscle lengthening, with a low complication rate. Proximal medial gastrocnemius recession showed comparable effectiveness and lower morbidity than Achilles tendon lengthening.
Conclusion: Posterior muscle lengthening is an effective intervention for treating equinus and related conditions, with technical variations allowing the procedure to be tailored to the patient’s etiology and clinical profile. Gastrocnemius recession appears to be a safe alternative with good functional outcomes, particularly in populations at higher risk for complications.
Keywords: Achilles tendon, soleus, gastrocnemius, surgical treatment, effectiveness, systematic review
Resumen
Introducción: El alargamiento de la musculatura posterior es una intervención quirúrgica empleada para tratar el equinismo y diversas patologías relacionadas con la limitación funcional del tobillo. El objetivo de este artículo es evaluar la efectividad y seguridad de las diferentes técnicas de alargamiento de la musculatura posterior (incluyendo Vulpius, Baumann, Strayer, Hoke, Z-plastia, Baker, Barouk, Silverskiöld) a través de una revisión bibliográfica.
Material y métodos: Se realizó una revisión sistemática de artículos científicos publicados hasta el año 2024, seleccionando aquellos que evaluaran los resultados clínicos, funcionales y quirúrgicos de las técnicas de alargamiento de la musculatura posterior de la pierna. Se incluyeron estudios experimentales, clínicos y revisiones que aportaran datos cuantitativos. En todos los casos se evaluó la calidad metodológica y el riesgo de sesgo mediante herramientas adaptadas al tipo de diseño de cada estudio.
Resultados: La mayoría de los estudios reportaron una mejora significativa en la dorsiflexión del tobillo y reducción del dolor tras el alargamiento muscular, con una baja tasa de complicaciones. La recesión proximal medial del gastrocnemio mostró efectividad comparable y menor morbilidad respecto al alargamiento del tendón de Aquiles.
Conclusión: El alargamiento de la musculatura posterior es una intervención efectiva para el tratamiento del equinismo y patologías asociadas, con variaciones técnicas que permiten adaptar el procedimiento según la etiología y características del paciente. La recesión del gastrocnemio se presenta como una alternativa segura con buenos resultados funcionales, especialmente en poblaciones con riesgo aumentado de complicaciones.
Palabras clave: Tendón de Aquiles, gastrocnemios, soleo, tratamiento quirúrgico, efectividad, revisión sistemática
Corresponding author
Alberto Rayo Martín
clinicarayo@gmail.com
Received: 23-07-2025
Accepted: 05-10-2025
Introduction
Lengthening of the posterior leg musculature, particularly the gastrocnemius and Achilles tendon, is a commonly performed surgical procedure used to treat various orthopedic conditions associated with equinus deformity and functional limitation of the ankle. These techniques, which include gastrocnemius recession and Achilles tendon lengthening, have become essential procedures to improve ankle dorsiflexion, relieve associated pain, and correct deformities that affect gait and quality of life(1).
Equinus deformity, characterized by a restrictive contracture of the triceps surae that limits ankle dorsiflexion, may result from multiple causes such as neurological disorders, metabolic diseases, or biomechanical alterations(2). In conditions like cerebral palsy, gastrocnemius contracture has been identified as a common cause of gait abnormalities leading to significant functional limitations. Several studies have demonstrated that both gastrocnemius recession and Achilles tendon lengthening can improve muscle length and function, resulting in a significant increase in ankle range of motion and enhanced limb function(4,5).
In diabetic patients with equinus deformity, the choice between gastrocnemius recession and Achilles tendon lengthening has particular clinical relevance. Greenhagen et al.(1) emphasized that gastrocnemius recession may provide substantial benefits in terms of forefoot pressure relief, with a lower risk of complications compared with Achilles tendon lengthening. This is especially important in the diabetic population, in whom wound healing and tissue integrity may be compromised. Moreover, a case report by the same authors(1,2,3,4,5)described a technical modification for performing proximal gastrocnemius recession as a safe and effective alternative for forefoot pressure reduction, underscoring the importance of appropriate surgical technique to optimize clinical outcomes.
In clinical practice, gastrocnemius recession has also been used to treat conditions such as metatarsalgia and chronic plantar fasciitis. Cortina et al. (5) reviewed the efficacy of gastrocnemius recession in patients with metatarsalgia, reporting significant improvements in pain relief and function by reducing forefoot tension. Similarly, Hoefnagels et al. (6) evaluated the effectiveness of gastrocnemius lengthening in patients with plantar fasciitis resistant to conservative therapy, showing increased dorsiflexion and reduced pain symptoms, supporting the use of this surgical intervention in selected cases.
From an anatomical and technical perspective, proximal medial gastrocnemius recession has been described as a technique that preserves muscle function and minimizes tissue damage, facilitating faster recovery and fewer postoperative complications(7). This procedure involves selective release of the medial belly of the gastrocnemius proximally in the knee joint, achieving increased functional muscle length without compromising Achilles tendon stability, thereby improving dorsiflexion without weakening the involved musculature.
Of note, the choice between gastrocnemius recession and Achilles tendon lengthening should be individualized and based on a detailed clinical evaluation that includes precise identification of muscle contracture and its functional impact. Isolated gastrocnemius limitation can be addressed through recession, while more global involvement of the triceps surae (soleus and gastrocnemious) may require tendon lengthening(8,9,10). In addition, factors such as age, etiology of contracture, and comorbidities must be considered to optimize surgical outcomes and minimize complications.
The present study focuses on the following clinical question: in adult patients with contracture or limitation of the posterior leg musculature, what is the clinical and functional effectiveness of gastrocnemius lengthening techniques compared with other interventions or baseline condition before intervention? This review aims to evaluate outcomes in terms of ankle dorsiflexion, pain relief, joint function, patient satisfaction, and postoperative complications, to provide evidence guiding the selection of the most appropriate surgical procedure for managing these musculoskeletal conditions.
Material and methods
We conducted a systematic review following the PRISMA 2020 guidelines to synthesize and critically analyze the available scientific evidence on the effectiveness of posterior leg muscle–lengthening techniques, particularly gastrocnemius recession, in various clinical conditions. The review was registered in PROSPERO under reference CRD420251151880.
For the present study a PICO question was formulated based in the following items:
Information sources and search strategy
The literature search was conducted in the following electronic databases: PubMed/Medline, Scopus, ScienceDirect,and the Cochrane Library.
The search period covered January 2015 to April 2025. Keywords and Boolean operators included: (“gastrocnemius recession” OR “posterior muscle lengthening” OR “Vulpius” OR “Strayer” OR “Baumann” OR “Hoke” OR “Z-plasty” OR “Baker” OR “Barouk” OR “Silfverskiöld”) AND (“plantar fasciitis” OR “metatarsalgia” OR “ankle dorsiflexion” OR “contracture” OR “arthrodesis” OR “gait” OR “biomechanics”).
Eligibility criteria and selection
Original human studies were included—clinical trials, cohort studies, observational studies, case reports, and relevant cadaveric studies—published in English or Spanish, evaluating the clinical or functional efficacy of posterior leg muscle–lengthening techniques. Studies were required to report outcomes such as dorsiflexion range, pain, joint function, complications, or patient satisfaction. Systematic or narrative reviews, letters to the editor, editorials, abstracts without full text, and studies unrelated to muscle-lengthening techniques were excluded. Procedures performed exclusively in pediatric or severely neuromuscular populations (e.g., cerebral palsy) were also excluded unless results were generalizable to the adult population.
Two independent reviewers screened titles, abstracts, and full texts according to defined criteria. Discrepancies were resolved by consensus or a third reviewer.
Data extraction and synthesis
Extracted data included: author and year, study design, surgical technique, patient population, treated disease, and clinical and functional outcomes (dorsiflexion, pain, satisfaction, complications).
Given the clinical and methodological heterogeneity of studies, techniques, and outcomes, a qualitative narrative synthesis was performed and meta-analysis was not conducted. Key findings were summarized in tables of characteristics and main results.
Quality assessment
Methodological quality was assessed using tools appropriate to study design. For non-randomized studies, the MINORS (Methodological Index for Non-Randomized Studies) was used. For observational and cadaveric studies, descriptive criteria focused on external validity and risk of bias were applied.
Results
Study selection
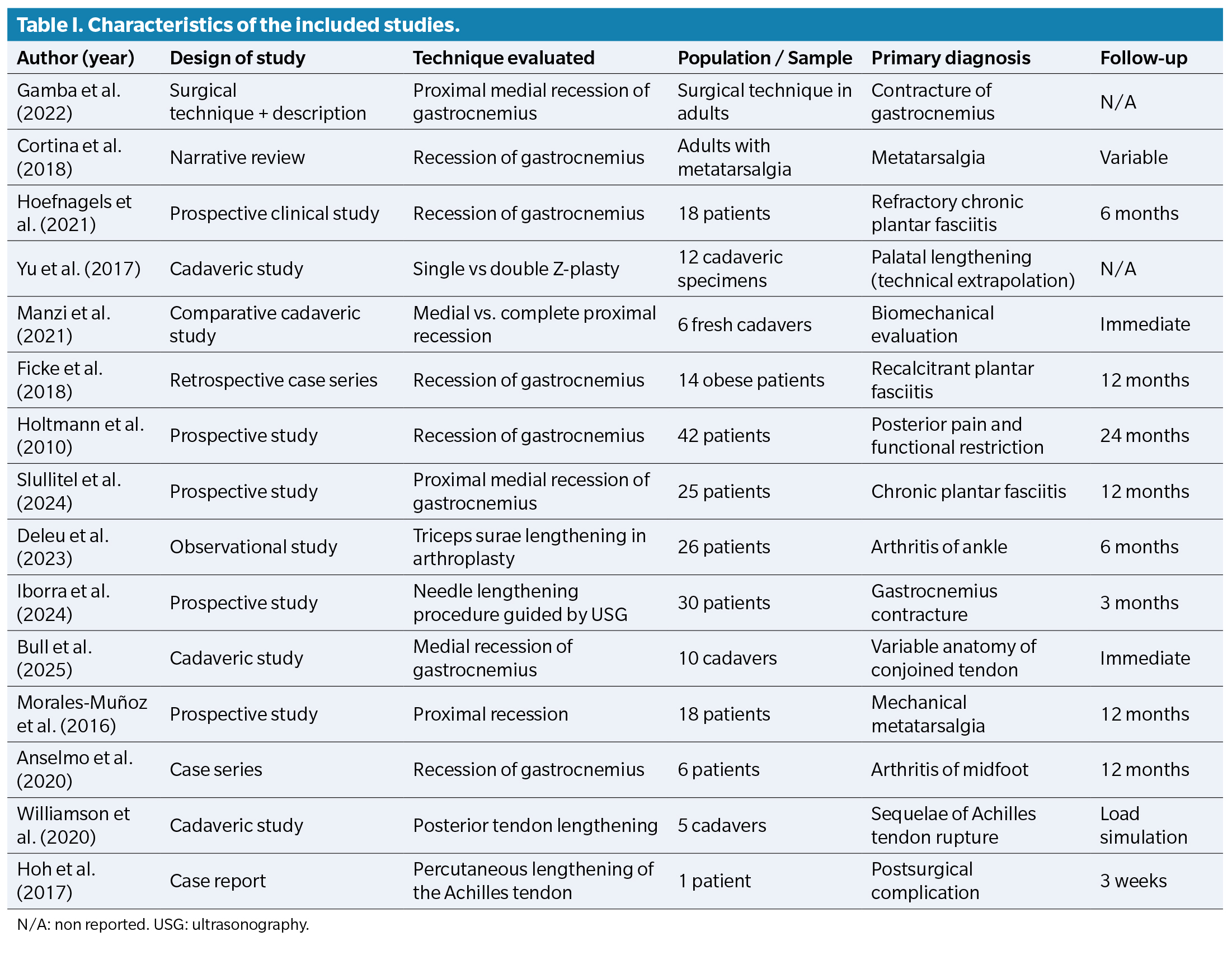
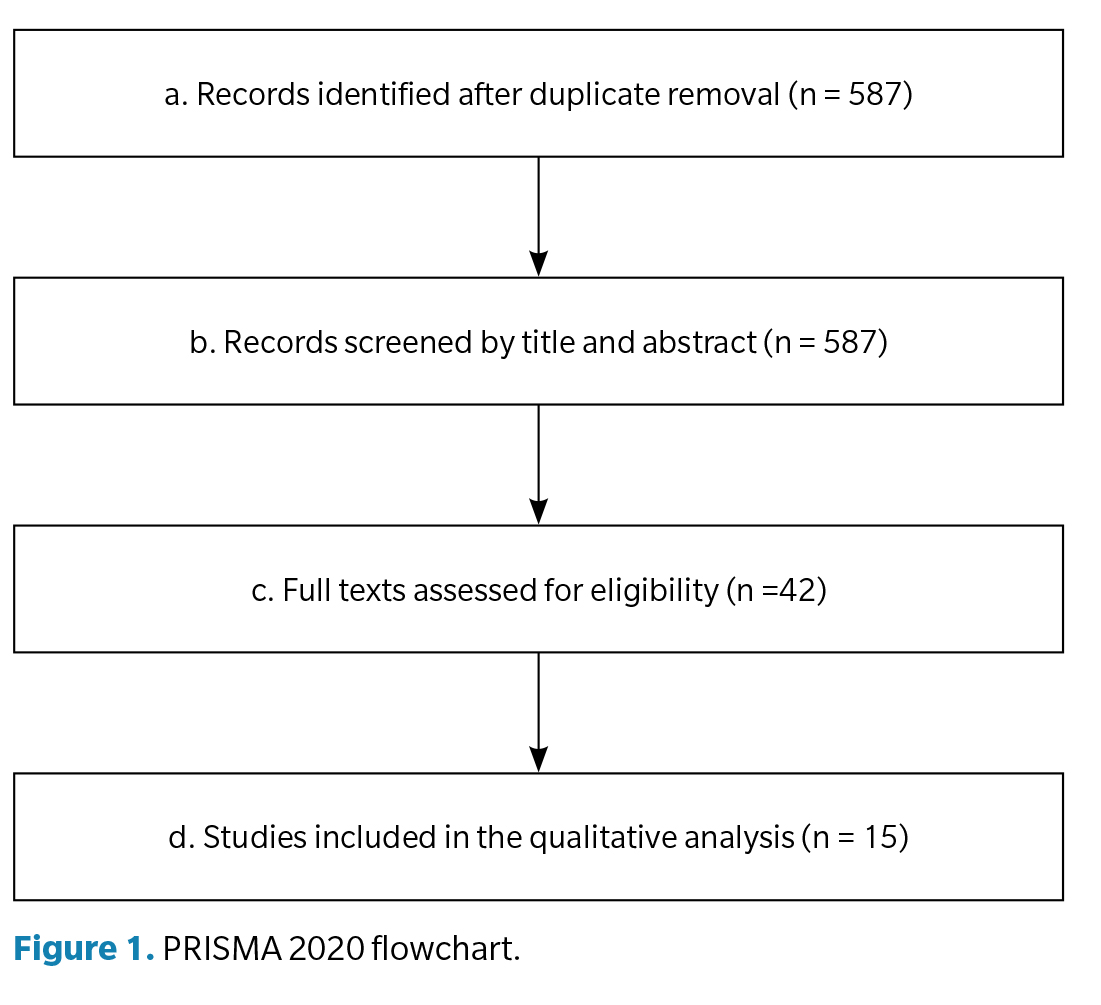
The search initially identified a total of 587 records after duplicate removal. After screening titles and abstracts, 42 full-text articles were reviewed. Finally, 15 studies (Table 1) met inclusion criteria and were included in the qualitative synthesis. The selection process is shown in the PRISMA 2020 flow diagram (Figure 1).
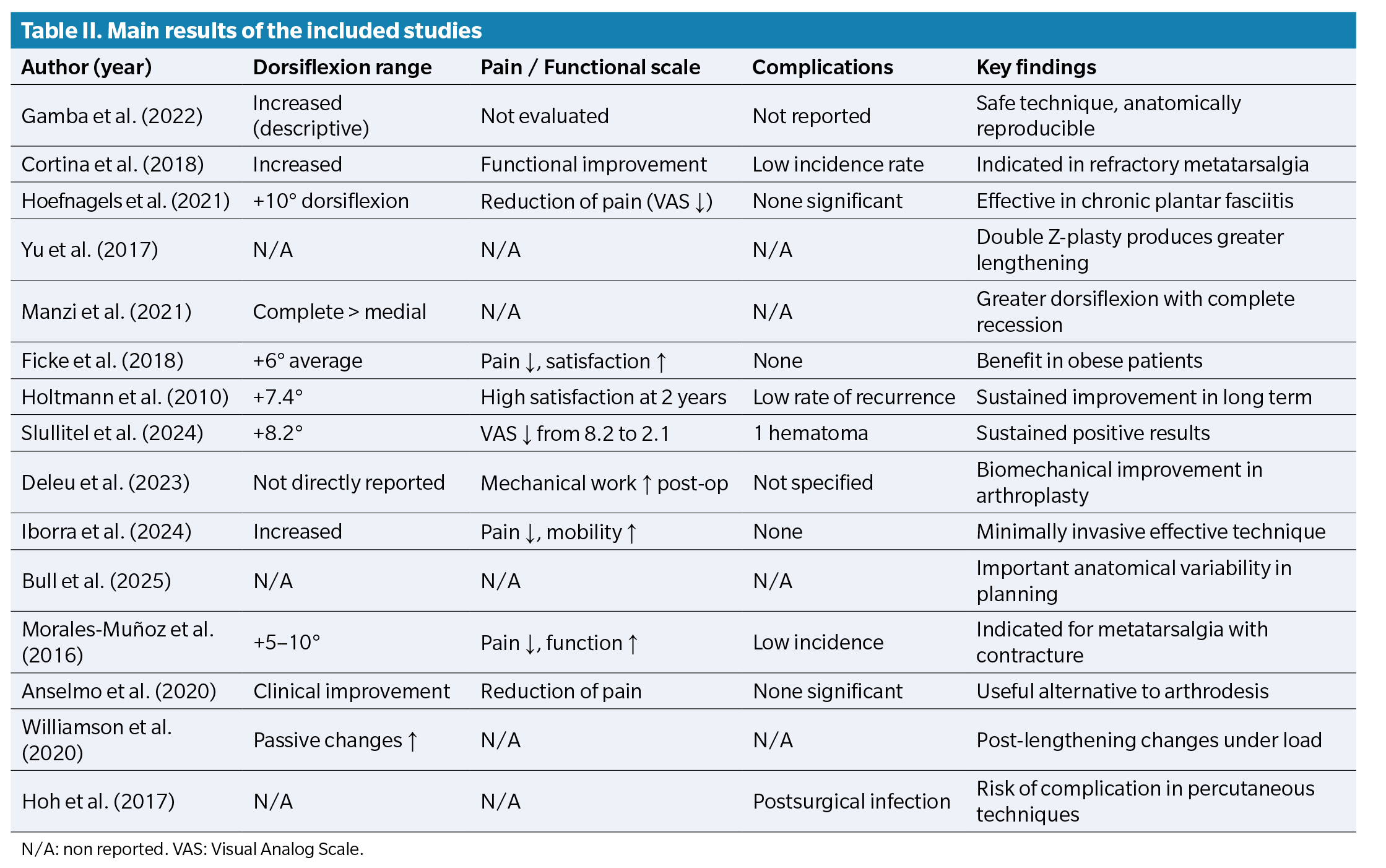
The included studies (Table 2) were published between 2016 and 2025, encompassing clinical trials, cohort studies, retrospective observational studies, cadaveric studies, and case reports. Populations included patients with conditions such as recalcitrant plantar fasciitis, metatarsalgia, gastrocnemius contracture, midfoot arthritis, and post–Achilles tendon rupture sequelae.
Most procedures were gastrocnemius recessions—mainly medial or proximal—along with variants such as Z-plasty and ultrasound-guided techniques.
Clinical and functional effectiveness
Both cadaveric and clinical studies showed significant improvement in dorsiflexion following gastrocnemius recession. In a cadaveric study, Manzi et al. (10) demonstrated that complete proximal recession provided greater dorsiflexion than isolated medial recession. Similarly, Greenhagen et al. (11) observed, after 2 years of follow-up, an average increase of 7.4° in ankle dorsiflexion in patients undergoing posterior muscle lengthening. Slullitel et al. (12) reported that patients with recalcitrant plantar fasciitis not only achieved increased dorsiflexion but also experienced significant functional improvement, highlighting the clinical benefit of these procedures.
Several studies reported significant pain reduction and functional improvement in patients with metatarsalgia and plantar fasciitis. Cortina et al. (5) and Morales-Muñoz et al. (13) observed substantial clinical improvement in mechanical metatarsalgia after gastrocnemius recession. Similarly, Hoefnagels et al. (6) and Ficke et al.14 documented pain reduction and enhanced functional capacity in chronic plantar fasciitis. Anselmo et al. (15) identified gastrocnemius recession as a less invasive alternative to arthrodesis in midfoot arthritis, emphasizing its safety and efficacy profile.
Complication rates were low across most studies. Hoh et al. (16) reported only a single postoperative infection following percutaneous Achilles tendon lengthening. Overall, procedures were well tolerated, with minimal risk of nerve injury or functional deficit—particularly when open controlled techniques were used—highlighting the safety of these procedures in experienced hands.
Comparison of techniques
Recent studies have explored technical variations in posterior muscle lengthening. Yu et al. (9), in a cadaveric study, compared single versus double-opposing Z-plasty, concluding that the latter produced greater tissue elongation—potentially applicable to gastrocnemius lengthening. Iborra et al. (17) proposed an innovative ultrasound-guided needle lengthening technique, showing promising clinical results with minimal invasiveness.
Biomechanical and functional impact
Several studies assessed the biomechanical effects of posterior muscle lengthening. Deleu et al. (18) demonstrated that triceps surae lengthening during total ankle arthroplasty modifies joint mechanical workload, suggesting improved load distribution. Similarly, Williamson et al. (19), in a cadaveric study, observed that posterior tendon lengthening produced significant passive changes in ankle joint motion under simulated load, supporting its potential to improve joint mechanics and functional tolerance.
Methodological Quality Assessment
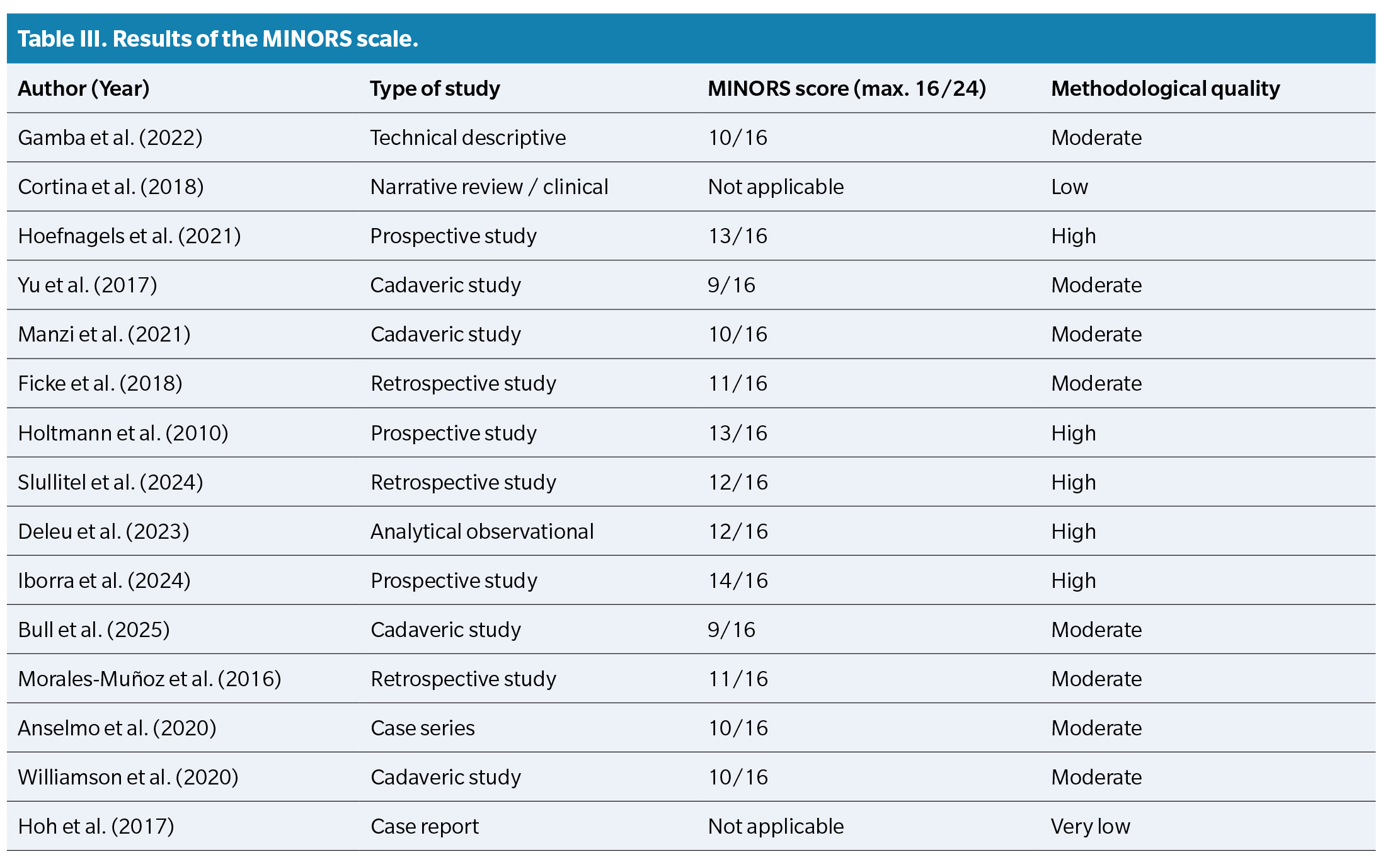
The MINORS scale (Table 3) was applied to assess methodological quality in non-randomized studies. It includes 12 items for comparative studies (maximum 24 points) and 8 for non-comparative studies (maximum 16 points), scored as: 0 = not reported, 1 = reported but inadequate, 2 = reported and adequate.
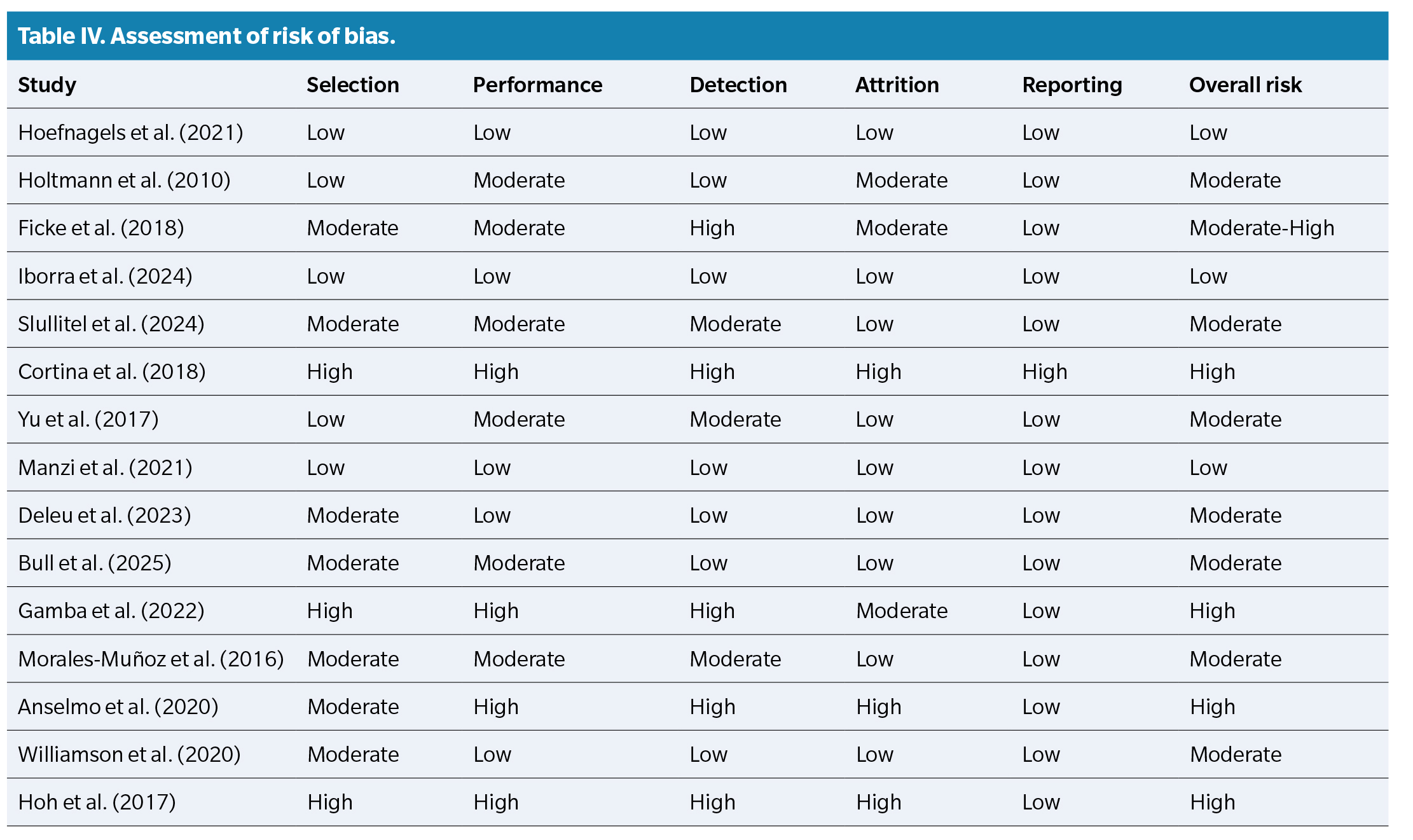
Risk of bias (Table 4) was evaluated qualitatively across 5 domains—selection, performance, detection, attrition, and reporting—and categorized as low, moderate, or high.
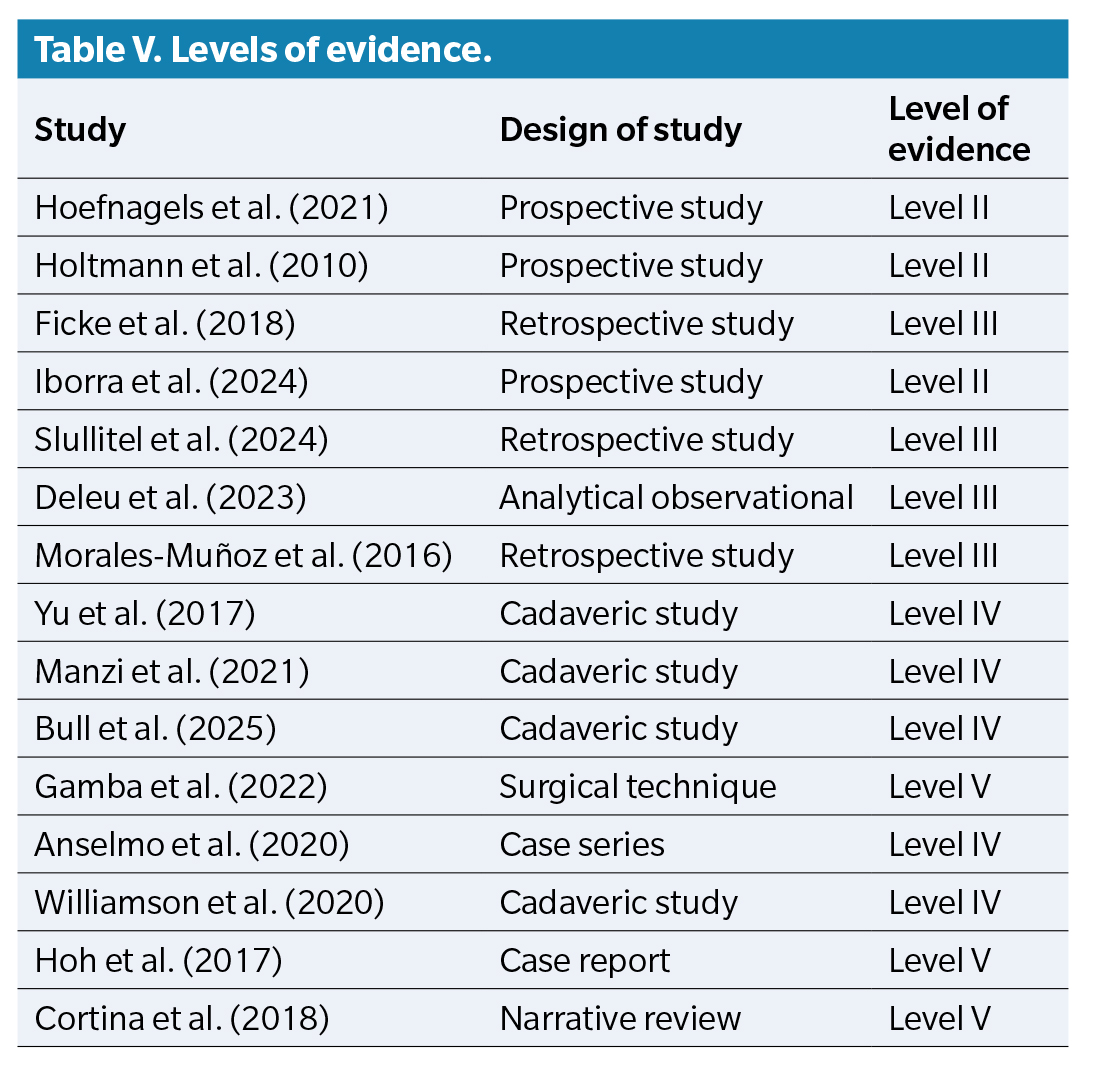
According to the Oxford Centre for Evidence-Based Medicine (2011) classification, evidence levels of the included studies are presented in Table 5.
Discussion
This systematic review compiles current evidence on the effectiveness of posterior muscle–lengthening techniques, mainly focused on the gastrocnemius, in musculoskeletal conditions such as plantar fasciitis, metatarsalgia, gastrocnemius contracture, and ankle arthritis. The diversity of surgical techniques—proximal medial recession (Vulpius, Strayer), Z-plasty, percutaneous and image-guided approaches—reflects a trend toward less invasive interventions with comparable outcomes to traditional methods.
Studies consistently reported improvements in ankle dorsiflexion, with mean increases of 5°–10°, as shown by Hoefnagels et al. (6), Slullitel et al. (12), and Greenhagen et al. (11). This functional gain is clinically significant, contributing to pain reduction and improved mobility in activities of daily living.
In chronic plantar fasciitis, gastrocnemius recession effectively reduces pain (as measured by VAS) and improves patient satisfaction, as demonstrated by Ficke et al.14 and Slullitel et al. (12). These findings support the hypothesis that excessive tension in the posterior chain may be a biomechanical factor perpetuating plantar pain.
Cadaveric studies, such as those by Manzi et al. (10) and Bull et al. (20), provide valuable anatomical and biomechanical insights. Manzi et al. demonstrated that complete gastrocnemius recession yields greater dorsiflexion gain compared with medial recession, whereas Bull et al. highlighted the variability of the conjoint tendon—an essential consideration in surgical planning to prevent iatrogenic injury.
Regarding complications, studies report a low rate of adverse events, with a few exceptions. Hoh et al. (16) described a postoperative infection following a percutaneous technique, underscoring the need for vigilance with minimally invasive approaches. Nevertheless, emerging techniques such as ultrasound-guided needle lengthening(17) have shown favorable outcomes without complications, making them a promising alternative in outpatient settings or in patients with contraindications to conventional surgery.
From a functional perspective, incorporating triceps surae lengthening in procedures such as ankle arthroplasty(14) has been shown to improve joint mechanical performance, which may have implications for implant longevity and postoperative functional outcomes.
Overall, the findings of this review support the use of posterior muscle lengthening as an effective, safe, and adaptable intervention across diverse clinical contexts. The choice of technique should be based on surgical experience, primary diagnosis, patient anatomy, and individual preferences. However, there remains a need for randomized controlled trials with stronger methodological rigor and long-term follow-up to strengthen the evidence base and establish more robust clinical recommendations.
This review has several limitations that should be considered when interpreting the results. The heterogeneity among the included studies regarding design, population, surgical techniques, and outcomes precluded the performance of a meta-analysis, restricting the synthesis to a narrative analysis. In addition, several studies had small sample sizes, short follow-up periods, or nonstandardized clinical outcomes, limiting the generalizability and comparability of the findings. The inclusion of cadaveric studies allows only anatomical or biomechanical inferences, making extrapolation to real clinical practice difficult. Similarly, the methodological quality of the studies was variable, with risks of selection, performance, and detection bias, and several studies presented low levels of evidence (levels IV–V). The restriction of the search to articles in English and Spanish and the potential omission of studies with negative results may have introduced publication bias. Taken together, these limitations suggest that although the available evidence indicates the efficacy and safety of gastrocnemius lengthening techniques, more robust data from prospective studies with larger sample sizes and longer follow-up are needed to confirm these findings.
Conclusions
Posterior leg muscle–lengthening techniques, particularly gastrocnemius recession, are effective in improving ankle dorsiflexion, reducing pain, and enhancing function in patients with chronic plantar fasciitis, mechanical metatarsalgia, gastrocnemius contracture, and ankle arthritis. These techniques show high postoperative satisfaction and an acceptable safety profile. Minimally invasive and ultrasound-guided techniques appear promising, providing efficacy with low morbidity. However, procedure selection must be individualized based on anatomy, underlying pathology, and surgeon experience. The current evidence, mostly observational and cadaveric, underscores the need for randomized controlled trials with larger samples and long-term follow-up to establish strong, evidence-based clinical recommendations.
Conflicts of interest
None declared
Funding
None declared
Contributions of the authors
Study conception and design: MAS, ARM. Data collection: RRM. Analysis and interpretation: RRM, AMRP. Manuscript drafting and preparation: MAS. Final review: AMRP
References